

Running Nightmares: Performance notes on how to run with ease
- Feb 25, 2019
- 17 min read

RUNNING DOES NOT HAVE TO BE PAINFUL!
Training for the London Marathon with plantar fasciatis? Doing the Couch to 5k programme with sore knees? Cross Country runner with lower back pain?
RUNNING DOES NOT HAVE TO BE PAINFUL!

Whilst this blog offers an extensive list of pain symptoms which can be incurred when running, it is NOT exhaustive, and it is NOT a list for self diagnosis - it is VERY IMPORTANT to seek diagnosis from a reputable physiotherapist as it is very complicated.
Therefore, this blog focuses on prevention and performance notes regarding how to avoid and rehab such pain symptoms. It is pretty easy too - it's just a case of having an understanding and being aware.
Pain does not have to be scary or stressful!
How to prevent running injuries and pains
There are a few things to understand first:
- Fascia: A connective tissue that provides cling film like properties to everything in the human body (albeit it can be found in all living things in various forms). Fascia has 2 main properties, 1) as it surrounds everything in the body, it reduces friction and keeps your body together through tensegrity, and 2) it's a big proprioceptive organ, meaning it absorbs pressure and provides feedback on this pressure to enable the muscles to react more efficiently. If you have ever prepared chicken, the white tissue which upon being peeled off the chicken becomes clear - that is fascia! There are different types of fascia for different purposes, such as the superficial fascia near the skin, to deep subcantaneous fascia in the gut. Plantar fasciatis is tension held in the fascia of the foot but the fascia does not stop there - it goes right up to the head. It is important to keep fascia hydrated and balanced functionally to reduce fascial tension so no matter what you do, for your fascia, the important part is HOW you do it!
If you're interested in learning more about this connective tissue, there is the British Fascia Symposium and the International Fascia Congress, as well as a plethora of research and literature. I recommend looking up Leon Chaitow, Gil Hedley, John Sharkey, Carla Stecco, Julian Baker, Susan Findlay and Caroline Barrow to name just a few.
- Your soft tissue is built like a matrix: thus running in all directions to enable your body to absorb pressures from any direction. Through postural and biomechanical dysfunctions/imbalances, the matrix begins to align to the strain as demonstrated through the Young's Modulus. As the tissue aligns to the strain, the body compensates by depositing more collagen to help stabilise and balance the area which reduces elastin capacity and therefore, reduces flexibility. A prime example of soft tissue matrix composition is trigger points!
- You have more than 1 diaphragm: Recent research has found that there is more than 1 diaphragm in the human body ranging from 4 to 12!!! A diaphragm is a transverse structure that separates an area into 2 compartments, and has a pumping mechanism which allows the diaphragm to move creating changing pressures within the compartments. The Dallas Osteopathy Study Group chaired by Dr. C. Speece discovered a potential 12 diaphragms in the body ranging from the arch of the foot, 2 in the knee, the pelvic floor, thoracic outlet and in the brain there is the tentorium cerebelli, and diaphragm sellae. Whilst there still needs to be much more research conducted to support these findings, it seems understandable that the human body would evolve to create such structures, particularly when we evolved to move vertically. Consider how the human body functions within gravity. These diaphragm mechanisms enable hydrostatic flow, improved balance due to increased proprioception, and rhythm which supports homeostasis. The function in one diaphragm could easily impact the other diaphragms which would be both advantageous in stressful situations, but disadvantageous with chronic stress and poor posture.
- Leg length differences: Leg length differences are much more common than you think, about 75% of my clients and athletes have a leg length difference. Whether someone experiences pain or injury caused or influenced by the difference is purely subjective, and therefore, it is important to see a professional who knows how to correctly measure leg length.

So having an understanding of those areas...
Feet
Supination/Pronation: As you move, your big toe should absorb 2-3 times your body weight. If you don't absorb it through the big toe, the foot absorbs it through the plantar plate (balls of the feet) and the instep (bones of the feet). This dysfunction can augment any supination or pronation depending on subjective elements.
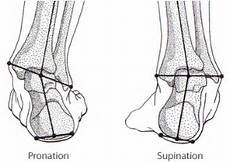









Big toe: Scientific name, the hallux (halluces: plural). Using the images above, it is easy to comprehend HOW you use your feet determines the structure of your feet. Bunions for example mean the big toe cannot absorb the pressure of movement as functionally as a straight big toe, which can increase pressure on the outside of the foot, and reduces function of the arch.
So for a functional foot to prevent such injuries and pains, use your big toe more and keep your feet straight - the big toe should be in line with your inner ankle as the muscles which rotate the leg outwards, i.e. toes pointing out, are in the glutes which causes misalignment and dysfunction through the leg into the foot. Think of the body as a building, if the foundations are not balanced and supportive, the structures above will struggle to maintain optimum function.
Exercises to help are towel scrunches, and practice curling the big toe with pressure ensuring feet are straight. A Strassbourg Sock can be helpful to stretch the fascia of the foot, and inserts such as a big toe straightener and plantar plate supports can help return the feet back to function.
For more information on the big toe and exercises, check out another blog: https://www.movewellnottingham.com/single-post/2019/03/14/Big-Toes-for-Big-Performance
For more information on the feet, check out another blog: https://www.movewellnottingham.com/single-post/2018/06/12/Plantar-Fasciatis-and-Carpal-Tunnel-FeetAnkles-HandsWrists
Knee
Being a hinge joint, pressures received by the knee depend on the foot/ankle and the hip, to which these depend on posture and biomechanics, noting the 2 diaphragms within the knee. Your patella (knee cap) should face forward, thus not inwards our outwards, to which the position of the patella can help determine current alignment. Too much pressure at the front of the knee is usually caused by an anterior tilt of the pelvis be it posturally or biomechanically and/or tight hip flexors and quads. There are 2 common knee dysfunctions through such pressure absorption, these being knee valgus and varus.




Valgus: Reduced support from the hip stablisers (predominantly gluteus medius and minimus), allowing the femur to medially rotate and collapse inwards at the knee causing weakness of the medial knee (signified by a weak vastus medialis obliquus - VMO), tension in the adductors, and increased pressure received by the arch in the foot/feet.
Varus: Tension in the hip causing a pull through the iliotibial band (IT Band), most commonly seen with a lateral rotation of the femur causing increased tension on the outer knee. This then can be seen with increased supination of the foot due to imbalanced pressures and alignment received by the ankle and foot.
Noting both knees do not have to be either valgus or varus, as it can differ between legs depending on posture and biomechanics.
For more information on the knee, check out my article written in collaberation with Safety in Sport Campaign: https://www.movewellnottingham.com/safety-in-sport-campaign-articles
Hips and pelvis
A fun little exercise that requires 2 people:
Standing facing each other, one turns their toes outwards so the leg is laterally rotated, and then the other gently pushes the one with the toes facing out at the shoulders. Compare the results with turning the toes inwards and again, the other gently pushes the one with toes inwards at the shoulders.
This exercise emphasizes the importance of foot position in regards to hip and pelvis balance.
Toes outward/feet laterally rotated: the big toe cannot absorb pressure functionally, meaning the outside of the foot attempts to maintain balance albeit not as successfully. This then means the outer knee receives increased pressure and the inner knee reduced pressure, causing the lateral rotators in the pelvis to absorb most of the pressure, bypassing the hip stabilisers. This means the spine receives more pressure than it should, resulting in reduced balance by pushing the centre of gravity higher.
Toes inward/feet medially rotated: the big toe can absorb most of the pressure, allowing the arch of the foot to receive and absorb such pressure. This then activates the inner knee structures such as VMO meaning the femur can translate such pressures functionally into the hip by activating gluteous medius and minimus. Therefore, through these hip stablisers, the pelvis is able to absorb the majority of pressure, reducing tension in the sacro-iliac joints (SIJs) and allowing the spine to receive this reduced pressure, enabling a functional centre of gravity.
Noting that whilst this position is more functional, it is meaningless without the use of the big toe/s.
Pelvic rotations: this can be both sides or just one. There is neutral positioning which allows optimum performance and thus reduced likelihood of injury and/or pain symptoms, yet there is also anterior rotation where the pelvis tilts forward, and posterior rotation where the pelvis tilts backwards. Whether the pelvis anteriorly or posteriorly rotates however, it signifies dysfunction of the abdominal and glute muscle groups as these work together to maintain a functional netural pelvic position. To prevent this, make sure hips are in line with ears and shoulders, and also knees and ankles. Using the glute muscles in ALL movement patterns is vital to prevent overloading of the hip flexors and groin which promotes anterior rotation.
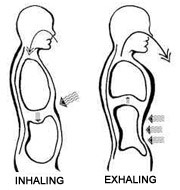
Breathing patterns: An easy way to help improve pelvic function and balance is to improve breathing patterns. When in rest, you should have a more diaphragmatic breathing pattern which requires the gut to move out on the inhale and back in on the exhale. Improved function of this respiratory diaphragm helps improve function and balance of the other 11 diaphragms.












For more information on the lower back and pelvis, check out another blog: https://www.movewellnottingham.com/single-post/2018/03/02/Lower-Back-Pain-and-Sciatica
Upper torso
Whilst there is little pain symptoms in this area which can be caused from running, 'stitches' being one of the few, this area is still important for function and performance when running.
Breathing patterns: Alike above, an easy way to help improve running performance is to improve breathing patterns. Babies commonly follow diaphragmatic patterns which can be seen in their gut moving in and out, yet by the time people reach adulthood, they rarely use the diaphragm and rather the thoracic cavity and collar bones absorb the pressure. More thoracic breathing patterns can be advantageous in short term when consideration is given to the requirements of the fight-flight-freeze response, yet long term it can be detrimental both mentally and physically. Thus, when in rest, you should have a more diaphragmatic breathing pattern which requires the gut to move out on the inhale and back in on the exhale. Improved function of this respiratory diaphragm helps improve function and balance of the other 11 diaphragms.
I find that dysfunctional breathing patterns can help induce cramp and 'stitches', increase MSK tension, influence more headaches, increases pressure on the shoulders, neck and head.
- For more information on the various breathing patterns, check out this other blog: https://www.movewellnottingham.com/single-post/2018/02/28/Stress-In-The-Neck-And-Shoulders
- For more information on stress and breathing patterns, check out this other blog: https://www.movewellnottingham.com/single-post/2018/11/06/The-Stress-Response-Why-breathing-patterns-matter
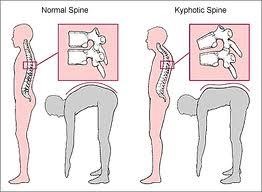
Head, neck and shoulder positioning: Imagine holding a heavy bowling ball in your hands with your arms out straight in front of you, and just stand there. It won't take long for your arms to feel sore, your shoulders and back to feel sore and tired, and you'll find yourself balancing on your toes to stop you from falling forward. Now that is how your neck feels when you keep your head tilted forward so that your ears are in front of your shoulders! POSTURE IS KEY TO STOP PAIN SYMPTOMS!
Neck muscles have been compared to the likes of hip flexors, more noticeable in sprinters when they require their neck to help them propel forward. However, the more tilted forward the neck is, the less support it can provide to such hip flexion as it is already flexed! So my top tips for this area to improve running performance and reduce chances of incurring pain symptoms:
- Shoulders rotated back and down away from the ears
- Head back so ears are in line with shoulders but keeping chin level (thus, don't tilt head back) - to prevent a 'sway back' posture, use your glutes and ab muscles.
- Run with your palms facing each other or toward the sky, not palms facing down as this weakens the arm through tension lines, and try to keep elbows in at the waist as they move back and forth.
- Breathe down into your gut as much as possible to utilise the more efficient areas of the lungs.












For more information on this area, check out another blog: https://www.movewellnottingham.com/single-post/2018/02/28/Stress-In-The-Neck-And-Shoulders
So to review the performance notes:
- use more big toe
- keep feet straight with inner ankle when pushing off big toe
- don't hyper-extend your knees
- use more glutes
- to stop you from tilting back through increased glute activation, use your abs to help you stand upright
- practice more belly breathing
- shoulders back and down
- ears, shoulders, hips, knees and ankles should all be aligned
- relax the jaw
Top Tip: warm up and down with resisted side walks.
What: Using a resistance band, wrap around ankles until there is a little resistance when standing square. And then walk sideways keeping both big toes aligned with both inner ankles at all times.
How: Upon increased resistance and fatigue, the feet will attempt to laterally rotate. To avoid this, focus on pushing down the big toe of the balancing leg whilst the other moves across. Do no compensate by allowing your foot to supinate. And finally, make sure knees are slightly bent and you move from the glutes and hips rather than the groin - if you feel it in the groin, you're not using enough glutes and big toes and probably have your pelvis anteriorly rotated.
Why: In my experience in sport and clinic, I find the gluteus minimus and medius the weakest of the pelvis muscles. Without strength and function is these muscles, the more pressure is put through the lateral rotators of the leg which can cause a variety of problems, including sciatica. They also help maintain function into the IT Band through TFL, and also the knee and foot.
Examples of running pains:
Feet
- Heel pain: inflammation of the calcaneous bursa which is a cushioning fat bad situated on the bottom of the heel to reduce pressure received by the calcaneous bone.
- Achilles tendonitis: strain of the achilles tendon which is the big tendon that runs down the back of the heel into the bottom of the foot (plantar section).
- Plantar fasciatis: tightening of the fascia on the plantar section of the foot (bottom of the foot).
- Heel spur: a small growth of bone which protudes out of the calcaneous bone.
- Plantar Plate pain: more commonly known as the 'balls of the feet', they can be inflamed with increased pressure, usually related to limited use of the big toe.
- Lateral foot pain: inflammation of the outer foot, most commonly at the plantar section, related to supination of the foot.
- Blisters: Blisters are caused by increased friction. To prevent them, make sure there are no creases in your socks, and you have comfy running shoes. They can be pretty annoying but from working in sport, I find the best ways to deal with blisters is with a blister plaster which is then secured using zinc oxide sport tape.

https://www.researchgate.net/figure/The-plantar-fascia-is-a-thick-band-of-connective-tissue-that-supports-the-foots-plantar_fig1_259577770
Lower leg
- Muscle tear: graded in severity, starting at the very small tears involving the tiny myofilaments which are Grade 1, Grade 2 which is an average tear involving one to a few myofibrils, to the more damaging Grade 3 tears which is complete severance of the muscle, usually located at the muscle-tendon junction.
Grade 1 symptoms: involving a mild ache and a mild stabbing pain when attempting to run, and little to no bruising.
Grade 2 symptoms: involving a deep ache with a deep stabbing pain sometimes in rest but especially when attempting to put pressure through it to move, and some bruising.
Grade 3 symptoms: involving severe pain even in rest, with no ability to put pressure through it when attempting to move. Recovery can happen without surgical intervention albeit rare, to which this MUST be discussed with a Consultant and Physiotherapist. A scan is required to check the condition of the surrounding connective tissue also.
- Achilles tendonitis: due to the position of this tendon, it can present pain in both the foot and lower leg. As above, it is a strain of the achilles tendon which is the big tendon that runs down the back of the heel into the bottom of the foot (plantar section).

Knee
- Patella tendonitis: The patella tendon inserts onto the superior anterior portion of the tibial tuberosity, to which increased tension in the quad muscles of the front upper leg can incur strain through the patella tendon. This causes inflammation and pain symptoms, especially when trying to flex the leg.
- Posterior knee pain: Hamstring tendonitis is tension in the hamstrings can cause strain of the hamstring tendons, but does not have to be related to muscle hypertrophy (increased muscle build). There are 3 hamstring muscles to which their tendons insert into the superior medial aspect of the tibia, and one has it's tendon insert into the superior lateral aspect of the fibia and lateral condyle of the tibia.
Popliteus overloading: can be related to strain of the hamstrings tendon/s, yet not necessarily. The popliteus muscle is a relatively small muscle which originates from the inferior lateral condyle of the femur, and inserts in a fan like fashion into the superior medial aspect of the tibia. This muscle promotes medial rotation of the knee joint, and also knee flexion. Thus, knee valgus can be a common cause of popliteus overloading.
- Outside knee pain: also known as lateral knee pain, this can be caused by tendons on the outside of the knee, and also the anatomy within the knee such as the lateral meniscus and cartilage.
Lateral collateral ligament strain: This ligament helps to stabilise the lateral aspect of the knee in posture and biomechanics. Severity of strain is graded similarly to muscle tears as above, ranging general inflammation, Grade 1 which involves one or two tears of ligament fibers, to Grade 3 which involves complete severance. Knee pain symptoms coincide with strain severity.
Medial collateral ligament strain: This ligament helps to stabilise the medial aspect of the knee in posture and biomechanics. Severity of strain is graded similarly to muscle tears as above, ranging general inflammation, Grade 1 which involves one or two tears of ligament fibers, to Grade 3 which involves complete severance. Knee pain symptoms coincide with strain severity.
IT Band strain/syndrome (causing pain at the knee): The IT Band, also known as ITB or iliotibial band, is a band of concentrated fascia forming from the tensor fascia latae situated on the outer hip, and inserts on the superior lateral (outside) aspect of the tibia. Tension in the hip can cause strain through the IT Band, which can cause a pulling sensation on the lateral aspect of the knee causing pain symptoms. Treatment SHOULD NOT be direct onto to the IT Band unless using myofascial release techniques, and rather focused on providing improved function in the hip and pelvis. How to prevent such pain is listed below these examples of running pains. For a more scientific explanation, Fairclough et al., (2006) provides a more in depth insight,
"The iliotibial band (ITB) or tract is a lateral thickening of the fascia lata in the thigh. Proximally it splits into superficial and deep layers, enclosing tensor fasciae latae and anchoring this muscle to the iliac crest (Standring, 2004). It also receives most of the tendon of gluteus maximus. The ITB is generally viewed as a band of dense fibrous connective tissue that passes over the lateral femoral epicondyle and attaches to Gerdy's tubercle on the anterolateral aspect of the tibia. ITB friction syndrome is an overuse injury well recognized as a common cause of lateral knee pain. It is particularly common in runners and cyclists, though it also occurs in weightlifters, skiers and soccer players (Orava, 1978; Noble, 1979; McNicol et al. 1981; Martens et al. 1989; Orchard et al. 1996)."
Fairclough J, Hayashi K, Toumi H, et al. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. J Anat. 2006;208(3):309-16.
- Inner Knee Pain: also known as medial knee pain, this can be caused by tendons on the inside of the knee, and also the anatomy within the knee such as the medial meniscus and cartilage.
Medial meniscus tear: Shaped like a horse shoe, it is a concentrated form of cartilage situated on top of the tibia (medial portion) to reduce friction between the tibia and femur in movement. Tears can appear in various forms graded similarly to muscle tears as above, and pain symptoms depends on severity. Whether surgical intervention is required or not should be determined by both Physiotherapist and Consultant.
Lateral meniscus tear: Shaped like a horse shoe, it is a concentrated form of cartilage situated on top of the tibia (lateral portion) to reduce friction between the tibia and femur in movement. Tears can appear in various forms graded similarly to muscle tears as above, and pain symptoms depends on severity. Whether surgical intervention is required or not should be determined by both Physiotherapist and Consultant.
ACL Tears: linking the medial anterior aspect of the tibia to the lateral posterior aspect of the femur, grading such tears are as any other ligament as discussed above. Most commonly caused by going from acceleration to immediate deceleration causing increased stabilising pressure through this ligament. Strengthening the hamstrings can prevent this but it is important to understand how and why which is discussed below the examples of running pain.
PCL Tears: linking the anterolateral aspect of the medial femoral condyle (within the notch) and the posterior aspect of the tibial plateau. Grading such sprains and tears are as discussed above. Injured most commonly when travelling from deceleration to straight acceleration with little joint support from both hip and ankle/foot. "The PCL is an important restraint of posterior tibial translation relative to the femur. In addition, the PCL acts as a secondary restraint to resist varus, valgus, and external rotation moments about the knee. While less common than ACL injuries, injuries to the PCL can occur from a posterior force directed on the tibia, most common with the knee in a flexed position" (Logterman et al., Posterior Cruciate Ligament: Anatomy and Biomechanics. Curr Rev Musculoskelet Med. 2018;11(3):510-514.

Upper leg
-Quad inflammation: There are 4 muscles which make up the Quadratus Group situated on the front of the femur which through overloading, can incur muscle tears as listed above in the lower leg section of this list. Muscle tears in this muscle are more common in the lower muscle-tendon junctions but can happen in the superior junctions and in the muscle body, and more strain symptoms can appear through overloading through the tendons and this can be common at both the superior and inferior quad tendons. Due to posture and modern day society being more stressful and requires more time sitting down and stress, such tension is usually related to hypertrophy through increased loading rather than due to atrophy.
- Hamstring inflammation: There are 3 muscles which make up the Hamstring Group situated on the back of the femur which through overloading, can incur muscle tears as listed above in the lower leg section of this list. Muscle tears can be common in both the lower and upper muscle-tendon junctions and sometimes in the muscle body. More strain symptoms can appear through overloading through the tendons and this can be common at both the superior and inferior quad tendons. Due to posture and modern day society being more stressful and requires more time sitting down and stress, such tension is usually related to atrophy rather than hypertrophy.

Hips and pelvis
- Sciatica: One of the most common pains, not just for runners, yet not many know what it is. The sciatic nerve originates from a collection of nerves in the lower spine from L4-S3 and they join before reaching the piriformis muscle in the pelvis. The sciatic nerve then runs down the back of the legs down to the feet. Pain symptoms can be local to the area of impingement, or can involve shooting pain up the back and down the leg. Due it's size, there are a number of causes from a slipped disc or bulging disc in the spine, tight sacro-iliac joints (SIJs) where the spine meets the pelvis, to a shortened piriformis which can compress the nerve causing pain symptoms. In clinic, I find the latter two are the most common causes.
- Lower back pain: This area is extremely complicated and thus diagnosing lower back pain must involve in depth assessments. Ranging from a slipped or bulging disc, tight SIJs, tight hip flexors, breathing dysfunctions, and generally poor posture and sitting down for long periods of time whether it be at a desk or driving. Pain can be localized or spreads across the lower back, and if left untreated, it can spread to the neck and shoulders, and/or down the legs.
The sciatic nerve is formed from the L4 to S3 segments of the sacral plexus, a collection of nerve fibres that emerge from the sacral part of the spinal cord.
For pain that is predominantly one sided, I advise getting a professional sports therapist to measure both legs for potential leg length discrepancy.




PLEASE NOTE: AS MENTIONED AT THE START, THIS LIST IS NOT EXHAUSTIVE! THE BODY IS EXTREMELY COMPLEX SO TO THINK THAT SUCH INJURIES COULD BE FULLY LISTED IS NAIVE.
DIAGNOSIS IS COMPLICATED.
REHAB IS COMPLICATED.
PREHAB IS NOT COMPLICATED - SO KEEP IT EASY AND LOOK AFTER YOURSELF BEFORE INJURY!
So running does not have to be painful, nor does pain have to be stressful!
Don't be a victim of your own body, take back control by learning about it in more depth.
- learn to understand it
- learn to be aware of it
- learn how to deal with it!
Kim is an Advanced Soft Tissue Therapist (BTEC Level 5: NLSSM). With extensive experience in both elite sport and private clinic, including performance, biomechanics and posture assessments, Kim has the ability and capacity to get you running again pain free!
Testimonial: Rich, a keen runner who had not been able to run due to chronic back pain for 9 years. This was after 1 treatment of 1 hour 30mins,
"Still feeling good after treatment. I even managed to go for a run the next day without any issues which was great. I haven't been waking up with a stiff or sore in my lower back since, especially if I've had an Epsom Salt bath the night before as you advised.I'm much more conscious about how I am walking at the moment and I think I am doing ok with that. I'm struggling with the breathing but I think that's going to take a bit of work and practice."
Kim has not needed to see Rich again as he has been pain free since.
For more testimonials: https://www.movewellnottingham.com/testimonials
So get in contact today, it's easier than you think!




















Comments