
PERFORMANCE SOFT TISSUE THERAPY CONSULTANT
BTEC L.5: NLSSM, 2013
- NOT JUST ANY SPORTS AND REMEDIAL MASSAGE -
HELPING PEOPLE SINCE 2013
PERFORMANCE IS FOR EVERYONE
- HIGHLY RENOWNED INTERNATIONAL REPUTATION -
Know Your Body
BLOG
RECOMMENDED THERAPISTS
SEARCH
BOOK CONSULTATION
RECOMMENDED READING LIST
MY ACCOUNT
YOUR PERFORMANCE
SECTION 6: ALIGNMENT
HIPS & PELVIS
HIP FLEXORS - THE ILIOPSOAS
Some of you may have heard about your hip flexors, often referring to the Psoas and Iliacus muscles, also known together as the Iliopsoas.
PSOAS MAJOR:
Origin: Bodies and transverse process of lumbar vertebrae
Insertion: Lesser trochanter (inside upper femur)
Action:
-
With the origin fixed (spine fixed):
-
Flex the hip (lifts leg upwards)
-
Potentially aid lateral rotation of the hip (coxal joint)
-
-
With the insertion fixed (leg fixed):
-
Flex the torso towards the leg
-
Anteriorly tilt the pelvis
-
-
Unilaterally assist to laterally flex the lumbar spine, so the left Psoas would help laterally flex the lumbar spine left for example.
ILIACUS:
Origin: Iliac Fossa
Insertion: Lesser trochanter (inside upper femur)
Action:
-
With the origin fixed (pelvis fixed)
-
Flex the hip (lifts leg upwards)
-
Potentially aid lateral rotation of the hip (coxal joint)
-
-
With the insertion fixed (leg fixed)
-
Flex the torso towards the leg
-
Anteriorly tilt the pelvis
-

FUN FACT: There is also Psoas Minor Muscles, but about 40% of the world population does not have them[i][ii]. This muscle aids posterior pelvic rotation, acting against Psoas Major, and is smaller than Psoas Major (hence the names). This muscle is most important in quadrupeds such as cats and dogs due to their relationship between spine and pelvis when moving on 4 limbs rather than 2. For notes sakes…
Origin: Body and transverse process of L1
Insertion: Superior ramus of pubis
Action:
-
Assist to create lordotic curvature in the lumbar spine (aiding spinal stabilisation)
-
Tilt pelvis posteriorly
[i] Anderson CN. Iliopsoas: Pathology, Diagnosis, and Treatment. Clin Sports Med. 2016 Jul;35(3):419-433.
[ii] Bordoni, B.; Varacallo, M. Anatomy, Bony Pelvis and Lower Limb, Thigh Quadriceps Muscle. Available online: https://www.ncbi.nlm.nih.gov/books/NBK531508/
The Iliopsoas is shortened whenever you flex your leg/knee upwards, or bend/tilt your torso forwards. Whilst this is great when standing and moving, modern society generally involves extensive periods of sitting down such as driving, desk work, sitting on a train/bus/plane, and relaxation such as watching television or going to the cinema. Therefore, modern society puts extensive postural pressure on the Iliopsoas, particularly the Psoas Major, and more so with laterally rotated legs, and especially with no Psoas Minor to offer further antagonistic support. Consequently, if a patient/client comes in with lower back pain, one of the first considerations is shortening of the Iliopsoas and Psoas Major hypertonicity as this can be a prime cause of lower back pain.










The psoas, the primary hip flexor, originates from the transverse processes of the lumbar vertebrae and can be a prime source of lower back pain. They are fast twitch muscles, making them a sprinters best friend (more on sprinters later), however, when tight, can cause a plethora of issues such as groin pain, adductor tension, and lower back pain as mentioned. Furthermore, there is a plethora of material that regard the psoas as ‘a storer of stress’, a key element of this is due to its close relationship with the diaphragm. The diaphragm originating from the L1-L2/3 and the Psoas originating from the bodies and transverse processes of the lumbar vertebrae, thus sharing the same origins at the top of the lumbar spine. Therefore, due to these relationships, tension can transfer, meaning if the diaphragm becomes tight, so can the Psoas Major and vice versa, which is why the Psoas Major is often considered when treating the MSK System in Respiratory Conditions.

There are many ways in which the Psoas can be impacted by dysfunctional breathing patterns. Firstly, think about what happens when you have a strong cough – your rib cage tilts forward thus tilting your torso forward – therefore engaging your hip flexors (with the insertion fixed). So already, a strong cough which can be caused by something simple as a mild cold, can cause the Iliopsoas to shorten, namely here the Psoas Major. Furthermore, in breathing patterns such as Thoracic or Clavicular breathing patterns, the rib cage absorbs the majority of pressure, not the gut, and this lack of diaphragmatic recoil into the gut not only causes tension to be transferred through to the Psoas, but creates increased tension into the neck and shoulders. This transferred tension thus influences a more kyphotic posture – we will come back to this in ‘Torso’ and ‘Upper Body’. However, as it is transferrable, postures such as kyphosis and lordosis can also create Respiratory symptoms such as shortened breaths, reduced intake on deep breathing, and therefore potentially associated symptoms such as reduced stamina and attention span.
There are many ways in which the Psoas can be impacted by dysfunctional breathing patterns. Firstly, think about what happens when you have a strong cough – your rib cage tilts forward thus tilting your torso forward – therefore engaging your hip flexors (with the insertion fixed). So already, a strong cough which can be caused by something simple as a mild cold, can cause the Iliopsoas to shorten, namely here the Psoas Major. Furthermore, in breathing patterns such as Thoracic or Clavicular breathing patterns, the rib cage absorbs the majority of pressure, not the gut, and this lack of diaphragmatic recoil into the gut not only causes tension to be transferred through to the Psoas, but creates increased tension into the neck and shoulders. This transferred tension thus influences a more kyphotic posture – we will come back to this in ‘Torso’ and ‘Upper Body’. However, as it is transferrable, postures such as kyphosis and lordosis can also create Respiratory symptoms such as shortened breaths, reduced intake on deep breathing, and therefore potentially associated symptoms such as reduced stamina and attention span.
NOTE
There can be a plethora of causes of lower back pain such as kidney infection, period pains, endometriosis, ruptured disc in the spine and tense muscles, of which the Psoas would be one of the first muscles to check. Furthermore, releasing the Psoas and thus lengthening it when the cause of lower back pain is a ruptured disc for example, it could make things worse as the Psoas Major has tightened in order to help protect the injured disc.
Therefore, it is important not to diagnose your own pain, there could many reasons why you are experiencing it, and rather use this information to generally help improve posture and biomechanics. If the pain eases and resolves through this improvement, then it was posture related pain and that correcting alignment and improving biotensegrity manged to ease hypertonic muscles and thus reduce compensations and dysfunction.
Regarding what to do when you have lower back pain, consider whether you are experiencing any other kind of symptoms and how badly it is affecting your day-to-day life, such as pain when going to the toilet (1s and 2s), difficulty doing any movement including breathing, numbness or pins and needles. If you are experiencing these symptoms, you must see a GP or Medical Health Professional as soon as possible, as if ignored, it could worsen symptoms and increase recovery time. For example,
-
If you are experiencing difficulty going to the toilet, or combined with difficulty breathing and moving, please dial 101 or see your GP, if it is severe, then dial 101 or emergency services.
-
If you are experiencing difficulty moving or combined with difficulty breathing, then a Physiotherapist, Osteopath, Chiropractor or Advanced Soft Tissue Therapist may be able to help, but again, if this is severe, then dial 101 or see your GP as soon as possible.
PSOAS CONNECTIONS
-
Haugstad et al (2006)[i] observed that women with chronic pelvic pain “typically displayed upper chest breathing patterns, with almost no movement of the thorax or the abdominal area”. They also confirmed “a characteristic pattern of standing, sitting, and walking, …lack of coordination and irregular high costal respiration”… and that “the highest density, and the highest degree of elastic stiffness [was] found in the iliopsoas muscles”.[ii]
-
Therefore, breathing patterns are vital for Iliopsoas functioning, with tension simultaneously increasing with dysfunctional chest breathing patterns. Haugstad et al (2006)[iii] also notes that “a specific pattern of pain, posture, movement, muscle pathology, and reduced awareness of one's own body was found in women with Chronic Pelvic Pain”, thus putting forward how posture and movement is important to help prevent Chronic Pelvic Pain, and also reduce Iliopsoas tension
-
-
Lee, Lee & McLaughlin (2008)[iv] have noted: “The abdominal canister is a functional and anatomical construct that synergistically work together [involving] the diaphragm, including its crura, and by extension the psoas muscle, whose fascia intimately blends with that of the pelvic floor and the obturator internus muscle, the deep abdominal wall including transversus abdominis, and its associated fascial connections, anteriorly and posteriorly, the deep fibres of multifidus, the intercostals, the thoracolumbar vertebral column (T6-12 and associated ribs, L1-L5) and osseus components of the pelvic girdle (innominates, sacrum and femora).”[v]
-
These findings suggest the Psoas has extensive fascial connectivity, including the pelvic floor, deep abdominal wall, transverse abdominis (whose responsibility is to help maintain abdominal tensegrity, thus, compress abdominal contents), spinal rotators, thoracic spine T6-T12 and their associated ribs, L1-L5 and sacrum. Consequently, Psoas tension can become widespread, eventually impacting the whole body. Furthermore, they also state that the function of the abdominal canister (your core) depends on how synergistically it works together including the Diaphragm and Psoas, putting forward that function depends on balance and cadence. The more balanced we are, the more we move with cadence, the more synergistically the abdominal canister can function.
-
From these 2 quotes alone, it is clear that Psoas Major is extensively connected, is an important factor for abdominal canister function, and can store extensive increasing amounts of tension through compensation, whether it is breathing and/or postural and/or biomechanical. Therefore, it is one of the most important muscles in the body for overall function.
[i] Haugstad G Haugstad T Kirste U 2006 Posture, movement patterns, and body awareness in women with chronic pelvic pain. J Psychosom Res. 61(5):637-644
[iii] Haugstad G Haugstad T Kirste U 2006 Posture, movement patterns, and body awareness in women with chronic pelvic pain. J Psychosom Res. 61(5):637-644
[iv] Lee D, Lee LJ, McLaughlin L. Stability, continence and breathing: The role of fascia following pregnancy and delivery. JBMT 2008;12:333-48.
[v] https://leonchaitow.com/2010/12/13/soft-tissue-manipulation-and-pelvic-pain/
THE GLUTES
GLUTEUS MAXIMUS
Origin: Coccyx, edge of Sacrum, Posterior Iliac Crest, and Sacrotuberous and Sacroiliac Ligaments
Action:
-
All fibers
-
Extend the hip
-
Laterally rotate the hip
-
Abduct the hip
-
-
Lower fibers:
-
Adduct the hip
-
You may have heard of your Gluteus Maximus, the biggest muscle in the body, it is the general antagonist to the Iliopsoas - the Iliopsoas shortening on hip flexion whilst the Gluteus Maximus lengthens, and the Gluteus Maximus shortening on hip extension whilst the Iliopsoas lengthens. Therefore, the best way to help prevent chronic tension in the Iliopsoas and consequential compensations and deviations which can impact the whole body such as an anterior pelvic tilt, is to increase Gluteus Maximus activation.
Furthermore, the Gluteus Maximus is generally considered a slow twitch muscle, and in conjunction with being the biggest muscle in the body, it is one of, if not the most important postural muscles. A prime example of Gluteus Maximus vs Iliopsoas function and balance is in Olympic sprinters (we will come back to Sprinting later).

Did you know there are 2 other Gluteus muscles making 3 in total? There is also Gluteus Medius and Gluteus Minimus, their names representing their size in relation to each other, thus, Maximus is the largest and Minimus the smallest.
GLUTEUS MEDIUS
Origin: Gluteal surface of the ilium, just below the iliac crest
Insertion: Lateral aspect of greater
Action:
-
All fibers:
-
Abduct the hip
-
-
Anterior fibers:
-
Flex the hip
-
Medially rotate the hip
-
-
Posterior fibers:
-
Extend the hip
-
Laterally rotate the hip
-
GLUTEUS MINIMUS
Origin: Gluteal surface of the Ilium underneath Gluteus Medius
Insertion: Anterior aspect of Greater Trochanter
Action:
-
Abduct the hip
-
Medially rotate the hip
-
Flex the hip


These muscles are vital for hip longevity and pelvic balance, and although small, you can see how Gluteus Minimus works for yourself...
All you need to do is stand up with feet pointing straight (so big toe aligned with inner ankle) and put your fingers on the tissue just behind the Anterior Iliac Crest – see video to help locate the point you need. Then curl your toes to scrunch your feet and do that a few times, and you should feel something move under your fingers – This is your Gluteus Minimus! Now do it with your feet pointing outwards, and you shouldn’t feel the Gluteus Minimus. What you are feeling is the Gluteus Minimus engage on scrunching your foot, however, it cannot work efficiently when the foot is turned outwards so you will not feel much if anything at all. In essence, this is what I describe to clients as the big toe to hip relationship.
INSIGHT: BIG TOE TO HIP RELATIONSHIP
Do you remember the ‘Food for thought’ at the start of this Section 6 which required 2 people – click here for a pop out window to re-cap:
(REQUIRES 2 PEOPLE)
To help people understand how simple postural changes can either help or reduce balance, Kim has a little trick and is based on the big toe to hip relationship.
To start, stand facing each other close enough to touch their shoulders. One of you moves your feet so they are pointing outwards, and the other GENTLY pushes them backwards on the shoulders and see how good balance is with feet pointing out. The person with the feet pointing outwards then points them inwards, and the other again GENTLY pushes them backwards on the shoulders and see how good balance is with the feet positioning compared to feet pointed outwards.
The concept is that balance SHOULD be better with feet pointed inwards (not necessarily the case all the time such as hypermobility can impact how well this works ). This therefore highlights the importance of alignment – and how this works will all be explained in this section!)
The above tasks help explain this relationship because when the feet are straight, your big toe and hip work together to absorb pressures, this transferring balanced pressures through the ankles and knees, meaning the pelvis can absorb the majority of force, enabling the spine to efficiently absorb and maintain stabilisation better. However, when the feet are rotated outwards, the more your quads are where your IT Band would be, your IT Band where your hamstrings would be, your hamstrings where your adductors would be and your adductors where your quads would be. In this position, the majority of pressure is placed on the outer foot (lateral longitudinal arch) and less down the inside (medial longitudinal arch), meaning the big toe is less able to efficiently absorb pressures as the outside leg and knee does this through compensation. Moving up, as the lateral rotators of the hip are engaged, the Gluteus Minimus is switched off, and also partially due to physics, the groin absorbs increasing pressure. As the Gluteus Minimus is unable to efficiently absorb pressures, the spine receives more pressure and if too much, can easily lose balance.
IN MORE FOCUS
What the arches are doing in someone’s feet can tell a therapist an awful lot, and combine this with the direction of the femur, and you gain a good idea as to how functional this big toe to hip relationship is, noting it can vary between feet/legs/hips. Check for patterns such as a medially rotated femur, laterally rotated feet, and fallen arches, or laterally rotated feet, tight Peroneals, and pronated feet. Both of these patterns can influence weakness in Gluteus Minimus, including the initial example despite the medially rotated femur because the supinated arch means little hip support from the big toe and thus medial longitudinal arch.
I teach this trick in more depth for my Martial Art and Weight Lifting athletes for example, feel free to book an Online Consultation for more information. In essence, you want to be strong in both positions, but for bodily alignment, the straight foot position for healthy pelvic absorption is paramount and not being strong in this posture means you will be dysfunctionally absorbing pressures with a posture of feet rotated out.
A good indicator of glute strength is the deep squat – being able to squat with your bum nearly touching the floor, and be able to stand up again without assistance. To achieve a deep squat, you need to be able to absorb forces between big toe, plantar plate and calcaneal (heel bone), allowing your Gluteus Minimus to engage the hip to reduce strain, and maintain balance between all 3 Gluteus muscles and the Iliopsoas to prevent tipping forward or backward, thus allowing your spine and head to help maintain equilibrium above the pelvis. Although it can be done, you should not need to rotate your feet out much to do this, and rather make your hips do some work instead.
Regarding your glutes, how you use your body, including posture, depends on how well ALL of your glutes can function. They should be engaged on standing up and walking, and you should be able to comfortably stand with straight feet and with each foot under each hip, not feet together. Your Gluteus Minimus may be small in size but that does not reflect its importance, as strength and mobility here is vital for overall pelvic and hip function and thus health.
With straight feet, look to see where your knees are pointing and whether you have supinated or pronated feet, as what they are doing will help discover where your glutes need work. This will assist in initiating a specific training plan for you, enabling you to focus on weaker areas with an aim to produce strength in good posture and biomechanics.
PELVIC ROTATIONS
BILATERAL
Imagine the pelvis is an oblong box supported by a pole either side to support the underneath (to resemble the legs), a tower of blocks stacked on top of each other which rises out from the centre of the back of the box (to resemble the spine). The balance of the box therefore depends on how well the structures below (poles/legs) and above (tower of blocks/spine) absorb postural and biomechanical pressures.
Some people use the bucket of water analogy to help explain pelvis balance. If the bucket tilts too far forward or backward, water would fall out. So, to keep all the water in the bucket, it is important to keep it balanced.
The concept of the pelvis tilting forward or backward can be related to overall posture, of which Kendall et al. (1983)[i] explains there are 4 predominant postural types:
[i] Kendall, F. P., McCreary, E. K., Provance, P. G., Rodgers, M., & Romani, W. A. (1993). Muscles, testing and function: with posture and pain (Vol. 103). Baltimore, MD: Williams & Wilkins. (BOOK)
LORDOTIC (anterior tilt)
-
Identified by an exaggerated curve of the lumbar spine.
-
Anterior pelvic tilt influences knee hyperextension and increased pressure down the front of the leg into the plantar plates of the feet, noting there is less ability to walk heel to toe efficiently, whilst straining the back of the leg. Due to the curve through the lumbar spine, there spine both above and below receive dysfunctional pressures which further the compensation. Regarding Anatomy Trains, this increases pressure on the Front Lines and strains the Back Lines.
-
Regarding muscles, the Quadratus Lumborum in the lower back is shortened restricting lower rib cage mobility, both Iliopsoas are very tight, both Quadriceps groups are hypertonic, and increased pressure through both sets of Peroneals. Regarding their antitheses on the other hand, the Abdominals are lengthened and weakened, noting increased pressures on the fibres of Transverse Abdominus, the Hamstrings are lengthened and weakened also, and the Gluteus Groups become generally weaker.

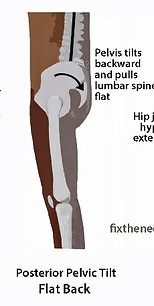
FLAT BACK (posterior tilt)
-
Identified by no curvature to the lumbar spine.
-
Posterior pelvic tilt influences increased pressure down the back of the leg causing more pressure down the calcaneus than the toes impacting calf and ankle pressures, noting there is less ability to walk from heel to toe efficiently, whilst lengthening and straining the front of the leg and the Abdominals. With no curve through the lumbar spine, there is extensive tension in the lower back and the spine above having to compensate greatly. Regarding Anatomy Trains, this puts increased pressure down the Back Lines whilst lengthening the Front Lines.
-
Regarding muscles, the Hamstrings and Abdominals are chronically shortened as is Psoas Minor if the individual has them, and the Glutes are absorbing more pressure than necessary. The Erector Spinae whose responsibility is to maintain spinal position are working overtime in a lengthened position, with the attachments to the lower back presenting chronically tight. Regarding the antitheses, the Psoas Major and Quadriceps are lengthened and strained, and breathing muscles compensate due to reduced ability to efficiently expand at the front causing increased pressure on the back of the rib cage.
SWAY BACK (forward shift and posterior tilt)
-
Identified by a forward shift of the pelvis which is also posteriorly rotated.
-
This is an extreme form of Flat Back posture which causes the spine to tilt backwards causing extensive compensation through the back, shoulders, neck and head, particularly as this posture influences ‘kyphosis’ through the upper back and neck (discussed in greater depth later in ‘Upper Body’. The combination of both a forward pelvic shift and a posterior pelvic rotation causes knee hyperextension, yet despite this, there is still increased pressure down the backs of the legs and excessive lengthening and strain down the front of the legs, also causing limited ability to efficiently walk heel to toe. As the Abdominals are lengthened, and Quadratus Lumborum and the lower portions of the Erector Spinae are chronically shortened, it places dysfunctional pressures throughout the thoracic cavity causing dysfunctional breathing patterns.
-
Regarding muscles, Psoas Minor is chronically tight if the individual has them, the Glutes are absorbing more pressure than necessary, and the Hamstrings are chronically shortened at their origin but chronically lengthened at the attachments, noting that despite their imbalance, they are absorbing excessive pressures. The Quadratus Lumborum in the lower back is shortened restricting lower rib cage mobility, and whilst the lower portions of the Erector Spinae Group are chronically shortened and tight, the upper portions are working overtime in a lengthened position. Regarding the antitheses, the Quadriceps and Psoas Major are chronically lengthened as are the Abdominals noting increased pressures on the fibres of Transverse Abdominus. As the Abdominals are lengthened, there is reduced ability to efficiently use the diaphragm in Diaphragmatic Breathing causing dysfunctional Breathing Patterns, augmenting the tension created in the back, shoulders, and neck.


BALANCED
-
Identified by a gentle forward curve of the lumbar spine, and the pelvis balanced between front and back. There is usually a relatively small difference between the highest point of the pelvis at the front, and the highest point at the back, the difference being completely subjective, yet is usually 4-5cm.
-
There is neither a posterior or anterior pelvic tilt as the pelvis is balanced, meaning normal pressures are being transferred and absorbed at both the front and the back of the body, including knee and ankle, allowing efficient walking from heel to toe. As there is pelvic equilibrium, there is the ability to efficiently breathe using the diaphragm and Abdominals, and thus influences normal pressures through the upper back, shoulders and neck. Overall, it influences equilibrium, efficiency, cadence, and exactly what the title states, balance.
-
Regarding muscles, this posture allows the slow twitch and fast twitch fibres to work efficiently, yet maintaining this posture requires effort to ensure no weakening into any such pelvic tilt. The Glutes and Hamstrings with their slow twitch fibres happily absorb the majority of postural pressure, and whilst the Quadriceps and Psoas Major ensure these muscles do not take over with an ensuing posterior pelvic tilt, they are somewhat lengthened and ready to move at speed if required. As there is a gentle lumbar curve, the lower back and Abdominals are balanced allowing efficient breathing patterns, thus the assisted breathing muscles are able to their other responsibilities efficiently and are ready to be engaged in case of an emergency such as stress or anxiety trigger, or sprinting for example.
As you will be starting to understand, posture means something different to each part of the body, yet they all share one thing in common, they all work best when they are balanced and thus, enjoy equilibrium. A balanced pelvis with no bilateral tilt means it influences equilibrium through to the knees, ankles and feet below, and the torso, rib cage, back, shoulders and neck above.
UNILATERAL
There is another kind of pelvic rotation and tilt, these are unilateral tilts, meaning each side of the pelvis is not tilting in the same way.
With regard to Anatomy Trains, these place varying pressures between left and right side between both Front and Back Lines, but also involves adaptation through the Spiral Line, Functional Lines, and Lateral Line. As this implies, there is extensive postural adaptation and therefore compensation.
There are many causes of a unilateral pelvic rotation, from bad posture and biomechanics to a spinal deviation such as Scoliosis or Torticollis, one side of the pelvis (the actual pelvic skeleton) may be smaller/larger than the other side, and Leg Length Differences, to name just a few. Consequently, the unilateral tilt may be a symptom of something else, to which a decent Physiotherapist, Osteopath, Chiropractor, Soft Tissue Therapist and/or Personal Trainer is the best course of action to treat such a rotation, although a combination of these therapists will get the best and quickest results.
To offer insight into Unilateral Pelvic Tilts, and the complicated nature of diagnosing and treating, here is some information on Leg Length Differences...


INSIGHT: LEG LENGTH DIFFERENCES/DISCREPANCIES
Classed under Limb Length Discrepancy (LLD), it is more common to have a limb length discrepancy than no discrepancy[i] with many people compensating for such differences as they can go unrecognised. Although arguable outdated, Knutson (2005)[ii] found that 90% of people in reviewed studies had an LLD. The most common direct difference being between 0.5cm and 1cm, however smaller and larger differences are not uncommon, yet some differences can be related to a pelvic rotation, thus, indirect, which will be discussed below.
Some people can go their entire lifetime with a limb length discrepancy and have no issues despite compensating, however, if someone does experience pain symptoms, considering limb length discrepancy is important to which it can easily be addressed to reduce pain symptoms. So what does this mean?
Go back to the start of 6:3 where the concept of pelvis balance is discussed. Imagine the pelvis is an oblong box again, supported by a pole at either to resemble the legs. Now imagine one of those poles being shorter than the other, meaning one side of the box is lower on one side. As one leg is shorter, and the other longer, the pelvis now receiving different pressures from either leg, some prefer to use their longer leg as their predominant leg, and others prefer to use their shorter leg. Not only are the various Anatomy Trains working harder to achieve balanced biotensegrity, but the overall body is.
[i] https://www.podiatrytoday.com/keys-recognizing-and-treating-limb-length-discrepancy (10 March 2020)
[ii] Knutson, G. A. (2005). Anatomic and functional leg-length inequality: a review and recommendation for clinical decision-making. Part I, anatomic leg-length inequality: prevalence, magnitude, effects and clinical significance. Chiropractic & osteopathy, 13(1), 11. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1232860/)
BELOW THE PELVIS
The feet will be absorbing varying pressures from above and the floor, with one foot dealing with more than the other, meaning varying pressures are translated up to the knee, and again, one knee dealing with more than the other. This then translates up to the hip where the pelvis either tilts or rotates to one side to compensate.
ABOVE THE PELVIS
As the pelvis tilts or rotates to one side, our eyes still want to face forward meaning the torso compensates to help absorb the varying pressures including gravity. The shoulder blades are no longer sitting on top of a balanced pelvis, meaning they too must compensate to absorb the varying pressures, and thus impacting the shoulder joint itself. Therefore, the positioning of the arms can be impacted meaning compensation and dysfunction can be translated through to elbow, wrist and the hand. The neck is now balancing the head on a body that is dealing with extensive compensation and varying pressures, to which the head may be tilting or rotating to aid its positioning to ensure the eyes face forward. If the head is rotating to compensate, suddenly one eye becomes closer to your foreground than the other, meaning eye muscles can be impacted as the eyes work to form a complete picture.
On the whole, the true extent of compensation and impact on the body is purely subjective meaning realistic statistics are difficult to collate, and there is no one rule fits all.

THERE ARE VARIOUS CAUSES FOR ALL PELVIC TILTS AND ROTATIONS, AND THEY CAN BE DIVIDED INTO THESE CLASSIFICATIONS:
-
CONGENITAL: Born with an LLI means the LLI is coded within your DNA. This can be passed on genetically by mother or father so it can be worth speaking to your parents and perhaps getting their legs measured.
-
DEVELOPED: Depending on growth rate and posture and biomechanics, our bodies can develop a LLI, and therefore this usually refers to a LLI through pelvic rotation rather than a direct difference. Growth is continuous until early 20’s for women and mid to late 20s for men and it is not uncommon for legs to grow at different rates, meaning throughout childhood, our bodies are constantly learning to stand and move with these changes, and sometimes the pelvis can rotate to adapt to such pressure changes. Moreover, posture and biomechanics throughout adulthood can also develop a LLI through pelvic rotation. Treating such a pelvic rotation requires the input of various specialised treatments including Osteopathy/Chiropractor/Physiotherapy with such Qualifications, Advanced Soft Tissue Therapy, Strength and Conditioning Training, and Physiotherapy can also be a good complement. Whilst this might seem like a lot, decent therapists will work together in accordance to your monetary and time availability, and resolving the issue properly from the start is important as building such strong foundations ensures longevity.
-
ACQUIRED: This can be related to medical conditions such as Osteoarthritis, injury, or surgical intervention. From this perspective, someone was not born with LLI coding, nor did they develop it through posture and biomechanics, and rather there was a specific event which caused the lengthening/shortening of a leg. As there is no ability to go back in time to check whether someone had a LLI before said event, it can be difficult to say whether this was acquired or not, and therefore seeing a decent therapist every so often can be good to make sure everything is ticking as it should. Moreover, as the LLI is acquired, it can be both a direct difference or via a pelvic rotation, meaning advice and treatment will depend on cause.
NOTE
A direct LLI can be resolved by a simple shoe insert such as a heel lift or full orthotic. It is VITAL that you get the right size for you so it is VITAL that you get measured and assessed by a highly reputable therapist who is experienced in measuring leg lengths. The therapist should also have a list of recommendations for such heel lifts/orthotics to save you from buying lesser quality products and spending more than required.
IN MORE FOCUS
Remember the notes on how collagen fibres can align to the direction of strain at the start of this Section, and how Anatomy Trains in Section 4 explains how the 7 trains adapt to each other allowing compensation despite dysfunction, well how your hold your pelvis in posture is paramount. Often used to help clients understand, imagine walking down a set of stairs with each of these pelvic postures, due to compensations effecting efficiency and function, the most balanced and thus less risk of injury is the ‘Balanced’ posture – the full bucket. For example, an anterior pelvic tilt increases strain on the back of the body, and increasing pressure on the front of the body, thus the torso compensates, creating difficulty to maintain efficient equilibrium which is important in reducing injury risk, especially when moving on inclines. Furthermore, walking up and down stairs with a unilateral pelvic rotation means both legs with be dealing with twists through their Anatomy Trains in order to maintain balance and looking forward, with the longer leg receiving more pressure due to hitching up through the hip, whilst the other hip is collapsed down and receives more pressure as a consequence – both legs are working hard to manage the dysfunction. Thus, with a unilateral pelvic tilt, both hips and legs are working hard to maintain balance for different reasons, whereas a bilateral pelvic tilt, both hips and legs are working hard to maintain balance for the same reasons.

INSIGHT: 100M SPRINT
The aim of the 100m sprint is to gain as much power as possible for a short amount of time and to do so, requires a perfect balance between forward and upward momentum, creating a smooth elastic spring that propels powerfully forward covering further ground per step. Whilst this is where the fast twitch muscles are in their prime, a predominant muscle group being the Quadriceps on the front of the upper leg, it is the Gluteus Maximus is a major player that enables the sprinter to remain as upright as possible to enable the fast twitch muscles to do their job efficiently. It is the Gluteus Maximus that helps to propel forward, and the Iliopsoas which helps to flex the hip (as the origin, the spine, is fixed in an upright position) bringing the leg up to create the upward spring.
With a deviation such as an anterior pelvic tilt for example, the Iliopsoas is already activated and shortened due to taking postural pressures and thus Gluteus Maximus is lengthened, therefore the potential power these muscles could produce is simultaneously reduced lowering potential speed.
Moreover, you will notice in top sprinters that as they take each foot off the floor, their heads move forward slightly, to which the Deep Front Line could help explain, and Julian Baker in his presentation at the British Fascia Symposium 2016 commented on how the Sternocleidomastoid muscles in the neck could also be classed as hip flexors under extreme pressure. Therefore, postures such as kyphosis will reduce potential output, and not just from a fast-slow twitch as kyphosis creates postural load to the front of the body and strain through the back, thus reducing Gluteus Maximus and Iliopsoas potential. Kyphosis also reduces respiratory capacity by reducing how much air you can intake per breath, noting also that the vagus and phrenic nerves pass through the neck to innervate the diaphragm and thorax. Hence, for your body to perform at the best it could be, posture and the biomechanics as a result of good posture is paramount.
For those interested, I highly recommend this video on the Olympic Youtube Channel by Michael Johnson (it will help ALL runners):
SCIATICA
The Sciatic nerve is formed by combining 5 lumbar and sacral spinal nerves, these being L4, L5, S1, S2, and S3. They come together to pass just in-front of the Piriformis where it continues down the back of the outer thigh where it branches off to form the Tibial and Peroneal nerves to eventually end at the foot and toes.
There can be many common causes of sciatica from a prolapsed disc in the spine, thus a disc between spinal vertebrae has slipped and is compressing on the sciatic nerve, to the Piriformis. If the pain is caused by a prolapsed disc, it can be extremely difficult to manage in the initial stages and if left untreated, it can get worse and, in some cases, the only option left is surgery. Consequently, it is absolutely vital that you seek advice from a health professional as soon as possible, if mild, it can be easily treated through a course of Physical Therapy with useful therapists including Physiotherapy, Soft Tissue Therapy, Osteopathy, Chiropractor and Strength and Conditioning/Personal Trainer. Thus, rather than worry and leave it hoping it will go away, just book an appointment and get it checked – simple, less worry, and you won’t have to suffer with pain for as long… so go get it checked, you only have one body so it’s important to look after it.

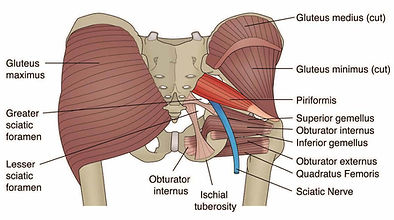
Regarding the Piriformis, as mentioned under Knee Varus earlier, it is one of the predominant lateral hip rotators. Put 2 and 2 together… if the hip is positioned in a laterally rotated position, the Piriformis is shortened, the more shortened it gets the more likely it can begin to compress on the sciatic nerve. Enter sciatica – the more the nerve becomes compressed/aggrevated, the more pain becomes a symptom. Shooting pain can be common and can be described as pain travelling down the leg and potentially into the feet, and also potentially upwards into the lower back, and also numbness in the bum cheek and down the leg. These can be either constant or intermittent, with intermittent pain usually shooting and/or increasing upon movement.
The diagnosis is important as if the tension in the glutes, lower back, and leg were to be released when the actual cause is a prolapsed disc, it could worsen the issue as the tension was there to help guard the disc. Consequently, if the Physiotherapist diagnoses the cause as the Piriformis, Soft Tissue Therapy is the best course of treatment to help resolve this issue, in conjunction with improving hip rotation which could thus include knee and foot positioning. A simple way to help reduce the pain in the short term is to sit/lie down and place a ball (the size of a tennis/hockey ball) under that glute, although preferably place one under each glute for pelvic balance as the opposite glute is usually tight also through compensating.
Overall, the best way to help PREVENT Sciatica, is to maintain straight feet and knees as much as possible, thus, both facing forward, and make sure to use your Glutes efficiently to ensure pelvic balance and spinal stability and strength. It can be that easy!
SPORTS HERNIA
TAKE THE QUIZ!
YOUR SCORE:
If you had issues answering any and got them wrong, don't worry, here are the answers with some info:
-
-
-
DONE!
DID YOU FIND THIS SECTION INTERESTING?
YES NO
DID YOU LEARN SOMETHING NEW?
YES NO
Again, better format with selection buttons. Information to be stored and used for website management.